Indications
Key indications include:
| Indication | Further information / rationale |
|---|---|
| Prolonged pregnancy (>41 weeks of gestation) | Prolonged pregnanices are associated with increased risk of stillbirth
Induction at 41 weeks (compared to 42 weeks) is associated with a reduction in perinatal mortality, neonatal intensive care unit admissions, and the likelihood of caesarean birth |
| PROM at term | Induction should be offered (see the PROM, P-PROM, and Preterm Labour article for more information):
Prolonged rupture of membranes increases the risk of infection. |
| P-PROM at 34-37 weeks | Patients are offered a choice of:
See the PROM, P-PROM, and Preterm Labour article for more information |
| Rupture of membrane with +ve GBS | Induction should be discussed to balance the risk of maternal or neonatal sepsis against the potential problems associated with preterm birth
Depends largely on the type of rupture of membrane and gestational age:
See the Group B Streptococcus in Pregnancy article for more information |
| Intrauterine fetal death | Induction helps manage the emotional and physical consequences of the death
Immediate induction is required if there is evidence of infection, bleeding, or ruptured membranes to protect the woman’s health |
Counsel women with previous Caesarean birth about the risks of induction of labour:
- Risk of uterine rupture
- Increased risk of emergency Caesarean birth
Assessment and Monitoring
Assessment Before Induction
| Assessment | Description |
|---|---|
| Assess fetal head position and engagement | Via abdominal palpation
If uncertain (e.g. breech suspected) → ultrasound |
| Vaginal examination to calculate the Bishop score | See details below |
| Cardiotocography | To confirm:
|
Monitoring During Induction
Once contraction begins after induction → offer cardiotocography monitoring
- If normal and low risk → switch to intermittent auscultation
- If abnormal fetal heart rate / uterine hyperstimulation → continuous cardiotocography + stop further induction doses and remove if possible
Methods of Labour Induction
Membrane sweep
Timing: routinely offer the woman an option of membrane sweeping after 39 weeks
Membrane sweep counselling:
- Procedure performed during vaginal examination: a finger is inserted into the cervix to perform a circular sweeping motion, attempting to separate the amniotic sac membrane from the uterine wall
- Underlying mechanism: this stimulates the release of prostaglandins which helps to soften and open the cervix
- Possible side effects: discomfort, light bleeding/cramping, but generally safe
Membrane sweep is NOT a formal induction method, but can reduce the need for formal induction (i.e. labour is more likely to start without the need for additional pharmacological or mechanical methods of induction).
Formal Induction Algorithm (Bishop Score-Guided)
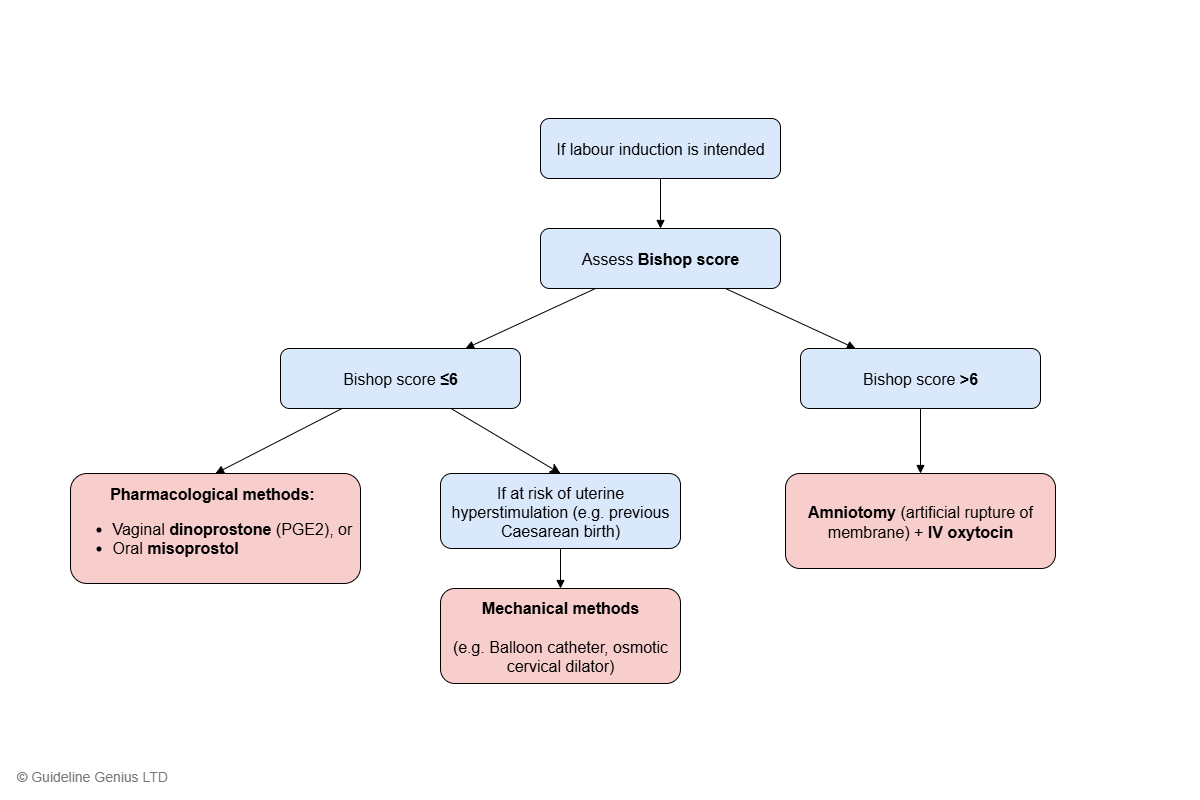
If labour induction is intended, the Bishop score is used to decide which method to use:
| Score | Cervix dilation (cm) | Cervix position | Cervical effacement (%) | Cervical consistency | Fetal station |
|---|---|---|---|---|---|
| 0 | 0 | Posterior | 0-30 | Firm | -3 |
| 1 | 1-2 | Midposition | 40-50 | Moderately firm | -2 |
| 2 | 3-4 | Anterior | 60-70 | Soft | -1,0 |
| 3 | ≥5 | ≥80 | +1,+2 |
Bishop score interpretation:
| Total score | Interpretation |
|---|---|
| ≥8 | Favourable / ripe cervix (i.e. cervix is ready to dilate), but NOT used to determine the choice of induction method |
| 6 | Unfavourable cervix
Cut-off used to determine the choice of induction method |
Bishop Score ≤6 → Cervical Ripening Methods
1st line: pharmacological induction methods
- Topical vaginal dinoprostone (PGE2) – tablet / gel / vaginal delivery system, or
- Oral misoprostol
Consider mechanical methods (e.g. balloon catheter, osmotic cervical dilator) if any of the following:
- High risk of uterine hyperstimulation and/or uterine rupture (e.g. previous Caesarean birth, multiple pregnancy, complex uterine scars, history of uterine rupture)
- Patient preference
Rationale: Bishop score ≤6 indicates an unfavourable cervix for labour, therefore cervical ripening methods are used to further prepare the cervix before active labour can be safely and effectively induced.
Bishop Score >6 → Labour Stimulating Methods
Offer induction with:
- Amniotomy, and
- IV oxytocin infusion
Rationale: Bishop score >6 indicates that the cervix is ripe and ready for labour, therefore there is no need to further ripen the cervix and labour can be directly stimulated.
Uterine Hyperstimulation
Uterine hyperstimulation is defined by:
- Tachysystole: >5 contractions per 10 min for at least 20 min, and
- Hypersystole / hypertonicity: contraction lasting ≥2 min
Management:
- Stop giving further induction medication
- Remove vaginally administered products if possible
- Perform continuous cardiotography
- Consider tocolysis
Hyperstimulation caused by misoprostol may be more difficult to reverse.
Mechanical methods are less likely to cause hyperstimulation than pharmacological methods.
Outpatient Labour Induction
For those who wish to return home, with no contraindications, consider:
- Topical vaginal dinoprostone (PGE2), or
- Mechanical methods
Ask the women to contact their maternity team if ANY of the following:
- Contraction begins
- No contractions in an agreed timeframe
- Membrane ruptures
- Bleeding develops
- Any other concerns (e.g. reduced fetal movement, excessive pain or contractions, side effects)
Simplified Flow Chart
Labour Induction Method Decision Algorithm