

Cervical Screening
Cervical screening is a national screening programme that aims to detect high-risk HPV infection and abnormal cervical cell changes before cervical cancer develops. It involves primary testing of high-risk HPV with reflex cytology and follow-up pathways such as repeat testing or colposcopy.
This updated high-yield UKMLA guide is based on the NHS Cervical Screening Programme, covers eligibility, frequency, results interpretation, screening pathways, and screening in special populations.
If cervical cancer is suspected clinically (e.g. abnormal vaginal bleeding), the cervical screening programme is intended only for individuals who are asymptomatic and otherwise well. It is not appropriate for these patients; they should be urgently referred, as discussed in the Cervical Cancer article.
Background Information
Purpose of the cervical screening programme: cervical cancer prevention – by identifying cervical intraepithelial neoplasm (CIN) early on, before it develops into cervical cancer.
Cervical Screening Test: HPV Testing and Cytology
In cervical screening, the Pap smear or smear test refers to the sampling method to collect cervical cells. The sample can then be used for HPV testing and/or cytology.
A Pap smear is performed in the clinic using a speculum to visualise the cervix, followed by the collection of cervical cells with a brush or spatula.
HPV Testing
HPV testing is the initial screening test of choice for cervical cancer, it tests for 14 high-risk HPV types (including 16 and 18 – the most carcinogenic ones)
Testing for high-risk HPV first is proven to be more sensitive than cytology.
Cytology
Cytology = microscopic examination of cervical cells, to look for abnormal cellular changes.
There are 3 possible cytology results:
- Negative: no abnormality detected
- Abnormal: the sample may show any of the following:
- Borderline changes in squamous or endocervical cells
- Low-grade dyskaryosis
- High-grade dyskaryosis (moderate)
- High-grade dyskaryosis (severe)
- Invasive squamous cell carcinoma
- Glandular neoplasia
- Inadequate: possible reasons for inadequate sample include
- Sample taken inappropriately
- Cervix not fully visualised
- Contains insufficient cells
- Contains obscuring element (e.g. lubricant, inflammation, blood)
- Incorrect labelling
Cytology can report dyskaryosis (cells with abnormal nuclei), but NOT cervical intraepithelial neoplasia (CIN).
CIN is strictly a histological diagnosis, made from a colposcopic biopsy or an excisional specimen. It assesses how much of the epithelial thickness is affected by abnormal cells.
Colposcopy
Colposcopy is a diagnostic procedure performed after abnormal screening results (i.e. Pap smear). It involves real-time visual examination of the cervix using a colposcope (magnifying instrument with light source).
The purpose of colposcopy is to obtain a biopsy of abnormal tissue to allow histopathological evaluation.
To identify abnormal tissue of the cervix that requires biopsy, the following techniques are often used:
- Application of acetic acid: stains abnormal tissue white (acetowhitening)
- Application of iodine: stains normal tissue dark brown
NHS Cervical Screening Programme
Target Population
ALL 25-64 y/o individuals with a cervix, regardless of gender identity
People with a subtotal hysterectomy still have a cervix, thus still need to undergo cervical screening.
Only those with a total / radical hysterectomy do not need to undergo cervical screening.
Frequency
Routine screening is performed every 5 years (assuming normal screening results)
From 1st July 2025 onwards, invitations are sent every 5 years across all ages (25-64 y/o).
Previously, cervical screening was offered every 3 years in 25-49 y/o and every 5 years in 50-64 y/o.
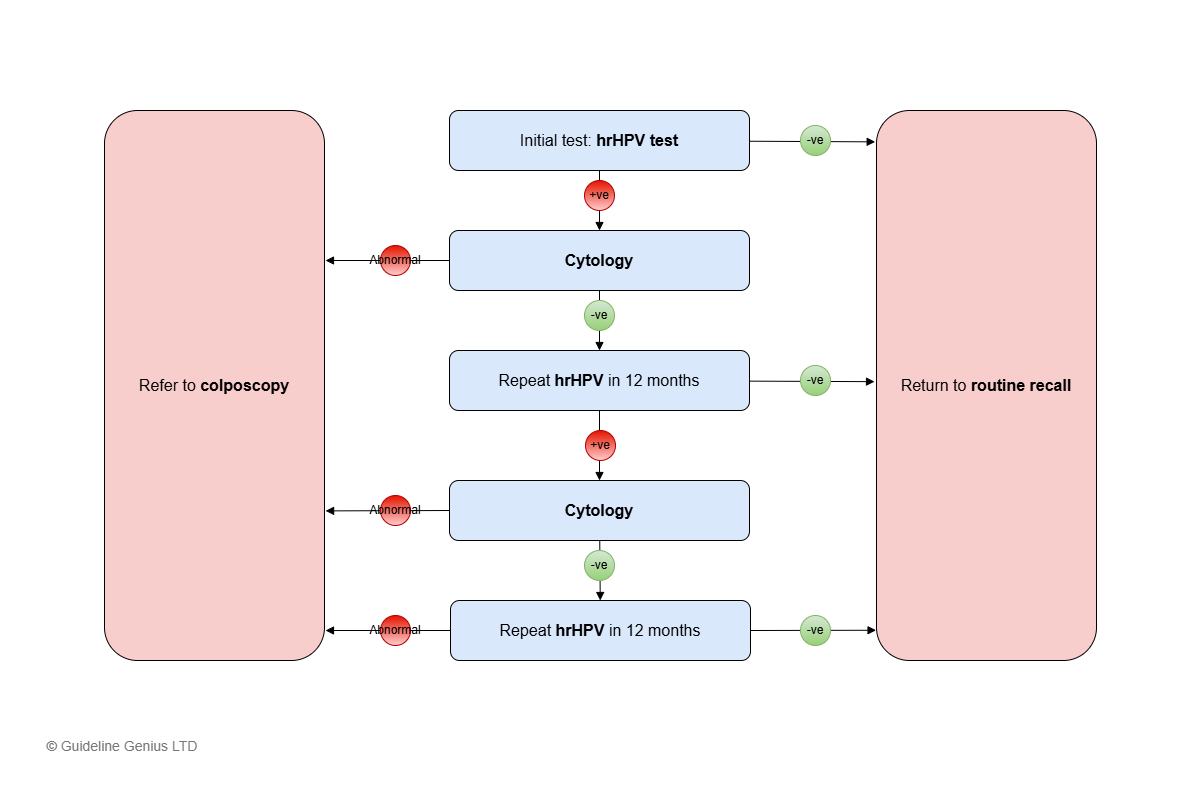
Standard Screening Algorithm (Most People)
The following algorithm applies to individuals attending routine recall with previously normal screening results.
Initial step: high-risk HPV (hrHPV) testing with reflex cytology (i.e. only perform cytology if hrHPV +ve, see below)
Subsequent steps depend on the hrHPV results.
-ve hrHPV
Return to routine recall (i.e. recall after 5 years)
+ve hrHPV
Perform cytology.
Subsequent steps depend on cytology results.
Abnormal Cytology Testing
Refer to colposcopy and biopsy
-ve Cytology (No Abnormalities)
Repeat hrHPV testing at 12 months.
Subsequent steps depend on the 1st repeat hrHPV results:
- 1st Repeat hrHPV -ve → return to routine recall (i.e. recall after 5 years)
- 1st Repeat hrHPV +ve → cytology testing
- Abnormal cytology → colposcopy referral
- -ve cytology → repeat hrHPV (2nd repeat) after 12 months
- 2nd Repeat hrHPV +ve (after 24 months) → colposcopy referral (irrespective of cytology results)
- 2nd Repeat hrHPV -ve → return to routine recall (i.e. recall after 5 years)
The screening pathway has 2 possible end outcomes:
- Return to routine recall, or
- Referral for colposcopy
After colposcopy (this is beyond the screening pathway), a summary of subsequent steps:
- Normal → further recall or discuss at MDT depending on hrHPV and cytology findings (NOT back to the routine recall after 5 years)
- Abnormal
- CIN → see the CIN article
- Cervical cancer → see the Cervical Cancer article
Unavailable HPV test / Inadequate Sample for Cytology
If this happens at any point → repeat the test after 3 months (no less than 3 months)
If still unavailable (HPV) results / inadequate cytology (that is, ≥2 consecutive times) → refer to colposcopy
Screening in Certain Populations
Reasons To Delay Screening
If any of the following:
- Menstruating
- <12 weeks after termination of pregnancy / miscarriage
- Currently pregnant and until 3 months postpartum
- Has vaginal discharge / pelvic infection
Screening During Pregnancy
Defer the test until at least 3 months postpartum
If previous cytology screening was abnormal and in the interim the person becomes pregnant:
- DO NOT delay colposcopy (can be done in the late 1st / early 2nd trimester)
- Only consider delaying assessment until after delivery if there are low-grade changes
Screening in Immunosuppressed Patients
HIV +ve patients → offer screening at diagnosis, then yearly screening (instead of 5-yearly)
Other immunosuppressed patients require screening at or near diagnosis/treatment, however, they don’t need more frequent cervical screening:
- Kidney failure patients who require dialysis → offer screening at or after diagnosis (if not up to date)
- Any other disease with high chance of needing organ transplantation → offer screening at or after diagnosis (if not up to date)
- Those about to undergo organ transplantation → offer screening within 1 year before transplantation
- Those who take cytotoxic drugs for rheumatological disorders → offer cervical screen at the start of treatment (if screening history is incomplete)
Simplified Flow Chart – Cervical Screening Pathway
References