

Background Information
HPV Testing Results
Cervical screening tests for 14 high-risk HPV types (including 16 and 18; the most carcinogenic ones)
Testing for HPV first is proven to be more sensitive than cytology.
Cytology Results
There are 3 possible cytology results:
- Negative: no abnormality detected
- Abnormal: the sample may show any of the following:
- Borderline changes in squamous or endocervical cells
- Low-grade dyskaryosis
- High-grade dyskaryosis (moderate)
- High-grade dyskaryosis (severe)
- Invasive squamous cell carcinoma
- Glandular neoplasia
- Inadequate: possible reasons include
- Sample taken inappropriately
- Cervix not fully visualised
- Contains insufficient cells
- Contains obscuring element (e.g. lubricant, inflammation, blood)
- Incorrect labelling
Cytology can report dyskaryosis (cells with abnormal nuclei), but NOT cervical intraepithelial neoplasia (CIN).
CIN is strictly a histological diagnosis, made from a colposcopic biopsy or an excisional specimen. It assesses how much of the epithelial thickness is affected by abnormal cells.
Colposcopy
Involves direct visualisation of the cervix with a colposcope
Common techniques / procedures performed in colposcopy:
- Application of acetic acid: stains abnormal tissue white (acetowhitening)
- Application of iodine: stains normal tissue dark brown
- Biopsy: to allow histological assessment
Guidelines
Target Population
Cervical screening target population:
- 25-64 y/o with a cervix regardless of gender identity
- Invitation sent every 5 years (assuming -ve screening)
From 1st July 2025 onwards, invitation is sent every 5 years across all ages (25-64 y/o).
Previously, cervical screening was offered every 3 years in 25-49 y/o and every 5 years in 50-64 y/o.
NB People with a subtotal hysterectomy still have a cervix, thus still need to undergo cervical screening.
Only those with total/radical hysterectomy do not need to undergo cervical screening.
General Screening Algorithm (Most People)
Initial screening test: high-risk HPV (hrHPV) testing with reflex cytology (i.e. only perform cytology if hrHPV +ve, see below)
-ve hrHPV
Return to routine recall (i.e. screen after 5 years)
Exceptions include:
- Test of cure pathway (post-CIN treatment): explained further down
- Untreated CIN 1 pathway
- The untreated CIN 1 pathway is different because CIN 1 is a diagnosed lesion requiring its own structured follow-up, not a routine screening scenario
- Due to low risk of progression, CIN 1 can be managed conservatively (vs CIN ≥2, which is actively treated on diagnosis) with follow-up:
- After diagnosis, ALL patients undergo repeat testing after 12 months, and further testing depending on results
- Only after 2 consecutive negative HPV results do they return to routine ‘screening’ recall (i.e., 5 yrly)
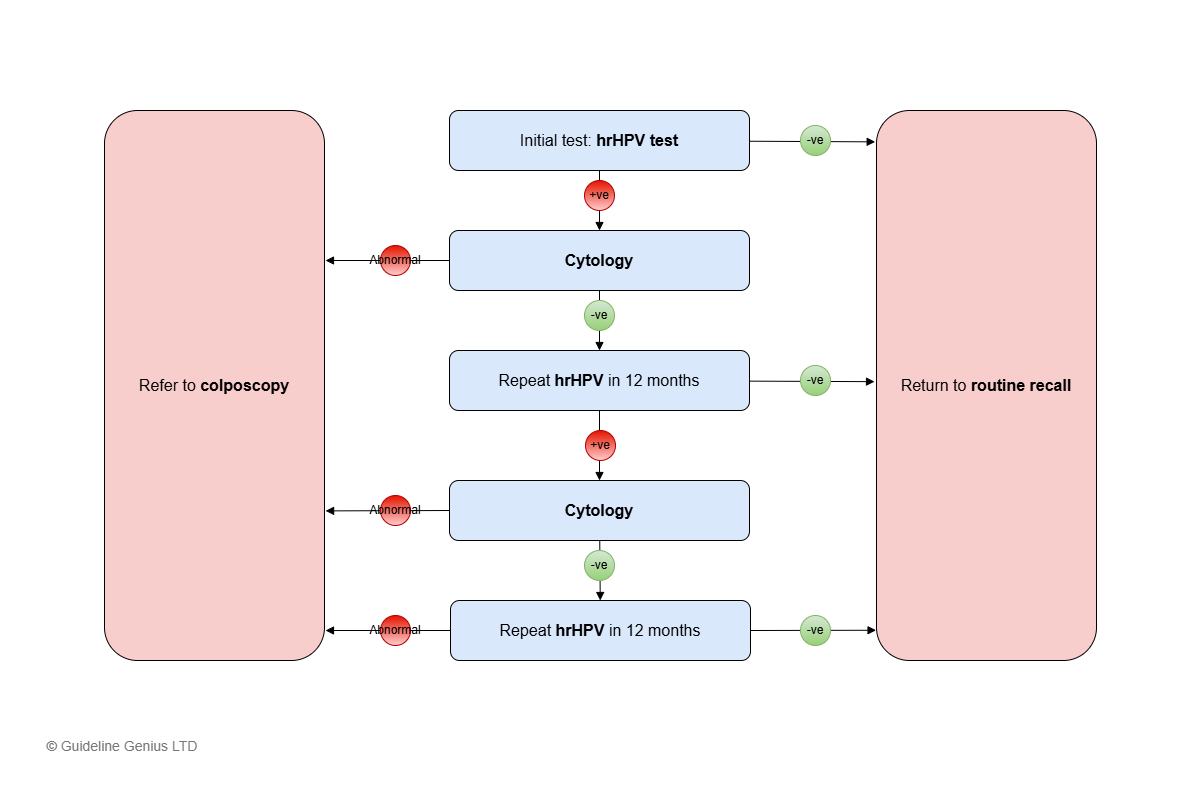
+ve hrHPV
Perform cytology testing.
Abnormal Cytology Testing
Refer to colposcopy
-ve Cytology Testing
Repeat hrHPV testing at 12 months
- hrHPV -ve → return to routine recall (every 5 years)
- hrHPV +ve → cytology testing
- Abnormal cytology → colposcopy
- -ve cytology → repeat hrHPV after 12 months
- hrHPV +ve (after 24 months) → colposcopy
- hrHPV -ve → return to routine recall (every 5 years)
To understand the interpretation and subsequent action from another angle, we are trying to stratify the patients into either 1) return to routine recall or 2) colposcopy
- hrHPV +ve alone is not an indication for colposcopy → do cytology first
- Whenever there is abnormal cytology → straight to colposcopy
- If there is hrHPV +ve but -ve cytology → repeat hrHPV (this is the 2nd time)
- If hrHPV becomes -ve → routine recall
- Again, following the above principle: if hrHPV +ve → do cytology, and if cytology abnormal → colposcopy
- But if cytology -ve for 2 times, and hrHPV still +ve (this is the 3rd time) → colposcopy
- Important: if cytology has been -ve, but hrHPV is still +ve at the 3rd time, colposcopy is necessary regardless of cytology results.
Unavailable HPV test / Inadequate Sample for Cytology
If this happens at any point → repeat the test after 3 months (no less than 3 months)
If still unavailable (HPV) results / inadequate cytology (that is, ≥2 consecutive times) → refer to colposcopy
Screening in Certain Populations
Reasons To Delay Screening
If any of the following:
- Menstruating
- <12 weeks postpartum
- <12 weeks after termination of pregnancy / miscarriage
- Currently pregnant
- Has vaginal discharge / pelvic infection
Screening During Pregnancy
Defer the test until at least 3 months postpartum
If previous cytology screening was abnormal and in the interim the person becomes pregnant:
- DO NOT delay colposcopy (can be done in the late 1st / early 2nd trimester)
- Only consider delaying assessment until after delivery if there are low-grade changes
Screening in Immunosuppressed Patients
HIV +ve patients → offer screening at diagnosis, then yearly screening (instead of 5 yearly)
Other immunosuppressed patients require screening at or near diagnosis/treatment, however, don’t need more frequent cervical screening:
- Kidney failure patients who require dialysis → offer screening at or after diagnosis (if not up to date)
- Any other disease with high chance of needing organ transplantation → offer screening at or after diagnosis (if not up to date)
- Those about to undergo organ transplantation → offer screening within 1 year before transplantation
- Those who take cytotoxic drugs for rheumatological disorders → offer cervical screen at the start of treatment (if screening history is incomplete)
Post-CIN Treatment
Perform test of cure (hrHPV test) 6 months after treatment:
- If hrHPV -ve → repeat cytology in 3 years
- If cytology -ve (after 3 years) → return to routine recall (i.e., 5 yearly testing)
If at any point hrHPV or cytology is +ve / abnormal → refer for colposcopy
Simplified Flow Chart
HPV screening Pathway
References