Background Information
Definition
Hyperkalaemia is defined as serum potassium ≥5.5 mmol/L
Classification of severity:
| Severity | Potassium concentration (mmol/L) |
|---|---|
| Mild | 5.5 – 5.9 |
| Moderate | 6.0 – 6.4 |
| Severe | ≥6.5 |
Aetiology
Given the extensive list of potential causes, memorising all of them is neither practical nor necessary. Prioritising the major causes and being able to recognise them in clinical practice is far more valuable.
Drug Causes
Drugs commonly implicated in hyperkalaemia
- RAAS inhibitor
- ACE inhibitor
- ARB
- Mineralocorticoid receptor antagonists (i.e. aldosterone receptor antagonist like spironolactone and eplerenone)
- Potassium-sparing diuretics (i.e., MRAs, amiloride/triamterene)
- NSAIDs
- Non-selective beta blockers
- Trimethoprim / co-trimoxazole
- Potassium supplements
Other Causes
- Acute and chronic kidney disease
- Hyporeninemic hypoaldosteronism (Type IV renal tubular acidosis)
- Adrenal insufficiency
- Pathological cell lysis (with release of intracellular K+ into the blood)
- Rhabdomyolysis
- Tumour lysis syndrome
- Haemolysis
Risk Factors
- Dialysis dependency
- Heart failure
- Diabetes
- Liver disease
ECG Changes
Progressive ECG changes seen in hyperkalaemia:
| Associated potassium levels | ECG changes |
|---|---|
| ≥6.0 mmol/L |
|
| ≥6.5 mmol/L |
|
| ≥7.0 mmol/L |
|
Pseudohyperkalaemia
Definition:
- Falsely elevated potassium levels
- Defined by serum potassium being >0.4 mmol/L higher than plasma potassium
Causes: mainly related to excess haemolysis during or after venipuncture
- Iatrogenic
- Prolonged transit time to laboratory / poor storage conditions – most common
- Prolonged tourniquet use
- Difficult/traumatic venipuncture
- Vigorous fist clenching
- ↑ Platelet count / erythrocytosis
If pseudohyperkalaemia is suspected:
- Repeat the blood test
- Send paired blood samples in a clotted tube (serum) and a lithium heparin tube (plasma)
Pseudohyperkalaemia should be suspected when hyperkalaemia is discordant with the clinical context.
Especially in the absence of symptoms, ECG changes, or risk factors for true hyperkalemia.
Management
Approach:
- Severe hyperkalaemia (≥6.5 mmol/L) → refer to hospital immediately
- Mild / moderate hyperkalaemia can generally be managed without hospital admission (if detected in the community), unless the patient is acutely unwell or has an AKI
Important: consider the possibility of pseudohyperkalaemia before initiating treatment for hyperkalaemia
- Pseudohyperkalaemia should be suspected when hyperkalaemia is discordant with the clinical context
- Especially in the absence of symptoms, ECG changes, or risk factors for hyperkalaemia
If pseudohyperkalaemia is suspected → repeat the blood test to confirm whether there is true hyperkalaemia
Primary Care Management
Management includes:
- Medication review (see above for drugs implicated in hyperkalaemia)
- Low potassium diet
- Consider a diuretic (loop or thiazide) if patient is non-oliguric and non-hypovolaemic
- Monitor serum potassium
Potassium binders (sodium zirconium cyclosilicate / patiromer calcium / calcium resonium) can be considered in:
- Moderate hyperkalaemia, and
- Patient with CKD 3b-5 (not on dialysis) or heart failure
Note that potassium binders should only be initiated in secondary care
Secondary Care Management
Summary Table
This table summarises the 3 main steps in the hospital management of hyperkalaemia, in order of urgency:
| Step | Aim and description | Recommended treatment |
|---|---|---|
| 1 (cardiac protection) | Only indicated if there are ECG changes
|
|
| 2 (potassium shifting) | Temporarily shifts potassium from extracellular to intracellular compartment to reduce serum potassium concentration |
Do not routinely give IV sodium bicarbonate for the acute treatment of hyperkalaemia |
| 3 (potassium removal) | Removes potassium from the body
Provides definitive correction of hyperkalaemia |
Potassium binders:
Other options:
|
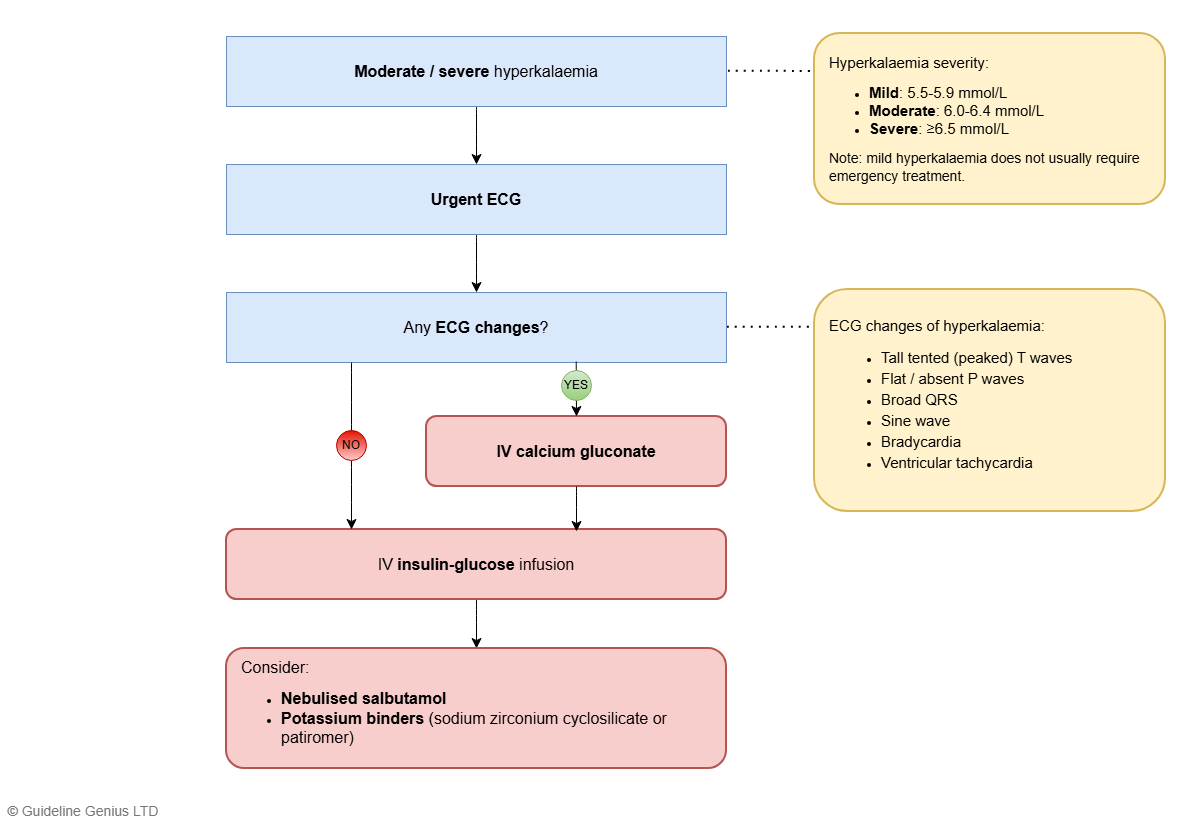
Emergency Management Algorithm
This section applies to BOTH moderate and severe hyperkalaemia (i.e. ≥6.0 mmol/L)
- If there is severe hyperkalaemia (≥6.5 mmol/L) → seek early senior input
- Note that mild hyperkalaemia (5.5-5.9 mmol/L) does NOT require any specific emergency treatment
If the patient develops cardiac arrest → ALS algorithm takes priority – Cardiac Arrest and Advanced Life Support (ALS) but treat the underlying hyperkalaemia in a similar fashion as below.
Step 1 (Immediate Management)
Perform an ECG urgently.
If there are any ECG changes (even if isolated tall tented T waves) → IV calcium gluconate 10% or IV calcium chloride 10%
- Consider a further dose if ECG changes persist after 5 min
- If there are no ECG changes → proceed to step 2
Note that current guidelines (UKKA, BNF, NHS GGC) did NOT make any recommendations on giving calcium gluconate / chloride if there are NO ECG changes. Click to see guideline rationale.
It is a common confusion that calcium gluconate / chloride should be given in severe hyperkalaemia (≥6.5 mmol/L), irrespective of ECG changes. Potentially arising from traditional teaching and MHRA authorisation.
Step 2
Offer treatment to lower serum potassium:
- ALL patients: insulin-glucose IV infusion (10 units of soluble insulin in 25g of glucose over 15-30 min), and
- Consider the following adjuncts:
- Nebulised salbutamol (10-20 mg)
- Potassium binders (sodium zirconium cyclosilicate / patiromer)
Monitor serum potassium and blood glucose throughout
If serum potassium remains ≥6.5 mmol/L despite medical therapy → seek expert help and consider dialysis.
Emergency Management Algorithm (Flowchart)
Disclaimer: This is a simplified flowchart for visual learning; some information has been omitted. See the ‘Emergency Management Algorithm’ section above for full details.