

Neonatal Jaundice
Jaundice is a yellow discolouration of the skin and sclerae due to the accumulation of bilirubin. Jaundice is newborn is common and is physiological in most cases. However, pathological jaundice may indicate a serious underlying cause.
Epidemiology
Jaundice is one of the most common conditions needing medical attention in newborn babies.
~60% of term and ~80% of preterm babies develop jaundice in the 1st week of life.
Neonatal Jaundice Classification
| Category | Definition / description |
|---|---|
| Pathological jaundice | Jaundice onset <24 hours after birth (jaundice within the 1st 24 hours is always pathological, but pathological jaundice can also present after 24 hours)
Other characteristic features:
|
| Physiological jaundice | Jaundice onset >24 hours after birth
Other characteristic features:
|
| Prolonged jaundice | Characterised by duration:
Prolonged neonatal jaundice is not automatically pathological. |
Key rules and relationships:
- Physiological jaundice may co-exist with pathological jaundice
- Conjugated hyperbilirubinaemia is always pathological, but not all pathological jaundice is conjugated
- Unconjugated hyperbilirubinaemia can be physiological or pathological
Causes
Pathological Neonatal Jaundice
Causes of jaundice with unconjugated hyperbilirubinaemia: [Ref]
| Cause | Key mechanism | Key clinical clues |
|---|---|---|
| Immune-mediated haemolysis (ABO or Rh incompatibility) | Maternal antibodies across the placenta → neonatal haemolysis → ↑ bilirubin production |
|
| RBC enzyme or membrane defects (e.g. G6PD, hereditary spherocytosis, pyruvate kinase deficiency) | Neonatal RBC abnormality → haemolysis → ↑ bilirubin production |
|
| Congenital hypothyroidism | Impaired hepatic bilirubin clearance + reduced gut motility → ↑ enterohepatic circulation |
|
| GI obstruction (e.g. pyloric stenosis, intestinal atresia, malrotation/volvulus) | Reduced intake/dehydration + reduced gut transit → ↑ enterohepatic circulation |
|
| Sepsis | Multifactorial: haemolysis, impaired hepatic bilirubin handling, and/or cholestasis |
|
| RBC sequestration (e.g. cephalohaematoma, subgaleal haemorrhage) | Breakdown of extravasated blood → ↑ bilirubin production |
|
| Crigler-Najjar syndrome | Inherited UGT1A1 deficiency → severely reduced or absent biliary conjugation |
|
Causes of jaundice with conjugated hyperbilirubinaemia: [Ref]
| Cause | Key mechanism | Key clinical clues |
|---|---|---|
| Biliary atresia | Fibro-obliteration of extra-hepatic ducts → impaired bile flow |
|
| Alagille syndrome | Lack of intra-hepatic ducts → impaired bile flow |
|
| Choledochal cyst | Congenital cystic dilatation of the bile ducts → impaired bile flow |
|
| Congenital / neonatal infections (e.g. TROCH infections) | Liver injury and/or impaired bile excretion |
|
| Alpha-1 antitrypsin deficiency | Misfolded alpha-1 antitrypsin accumulates in hepatocytes → liver injury and cholestasis |
|
| Galactosaemia | Inborn error of galactose metabolism → toxic metabolite accumulation → liver injury |
|
Physiological Neonatal Jaundice
| Cause | Key mechanism | Key clinical clues |
|---|---|---|
| Physiologic jaundice | Combination of various physiological alterations:
|
In a full-term baby, jaundice:
|
| Breastfeeding jaundice | Inadequate breast milk consumption → dehydration → ↓ intestinal motility → ↓ biliary excretion in the stool |
|
| Breast milk jaundice | Components in the breast milk reduce bilirubin conjugation and increase enterohepatic circulation |
Unlike breastfeeding jaundice, this occurs in infants who have adequate feeding and good weight gain |
Physiological jaundice may co-exist with pathological jaundice.
Complications
Only unconjugated bilirubin can cross the BBB and cause bilirubin neurotoxicity.
Severe unconjugated hyperbilirubinaemia can result in:
- Acute bilirubin encephalopathy: lethargy, irritability, poor feeding or poor suck, abnormal muscle tone, abnormal posture such as opisthotonus, high-pitched cry, apnoea, seizures, and coma
- Chronic bilirubin encephalopathy: permanent neurological consequences of bilirubin neurotoxicity
- Usually becomes apparent during 1st year of life
- Choreoathetoid cerebral palsy, seizures, developmental delay, learning difficulties, hearing impairment, visual problems, and dental enamel dysplasia
Kernicterus is a term used to describe the clinical features of severe bilirubin encephalopathy and the pathological finding of deep yellow bilirubin staining in the brain.
Conjugated bilirubin is water-soluble and does not usually cross the BBB.
Conjugated hyperbilirubinaemia (e.g. in biliary atresia) has negligible direct neurotoxicity. The main complications usually result from the underlying cause, such as cholestasis, biliary obstruction, or liver disease.
Investigations and Work-Up
The following investigations should be performed in neonatal jaundice to identify the underlying cause:
- FBC and blood film
- Serum bilirubin (conjugated vs unconjugated levels)
- Blood group (mother and baby)
- Coomb’s test
- LFTs
- Routine metabolic screening (including for congenital hypothyroidism, if not already performed)
- G6PD levels
If infection is suspected: cultures of blood, urine and/or CSF
Diagnosis and Assessment
Timing to measure serum bilirubin:
- Suspected/obvious jaundice < 24 hrs of life → measure within 2 hours
- Suspected/obvious jaundice ≥ 24 hrs of life → measure within 6 hours
There are 2 ways to measure bilirubin levels:
| Approach | Description | Indications |
|---|---|---|
| Serum bilirubin | Gold standard method (most accurate):
|
ANY of the following:
|
| Transcutaneous bilirubin | Screening method:
|
Only if ALL the following are present:
If transcutaneous bilirubin levels are elevated (>250 mmol/L or above the treatment threshold) → confirm with a serum bilirubin level |
Serum bilirubin (NOT transcutaneous bilirubin) is used to guide management of neonatal jaundice.
Management
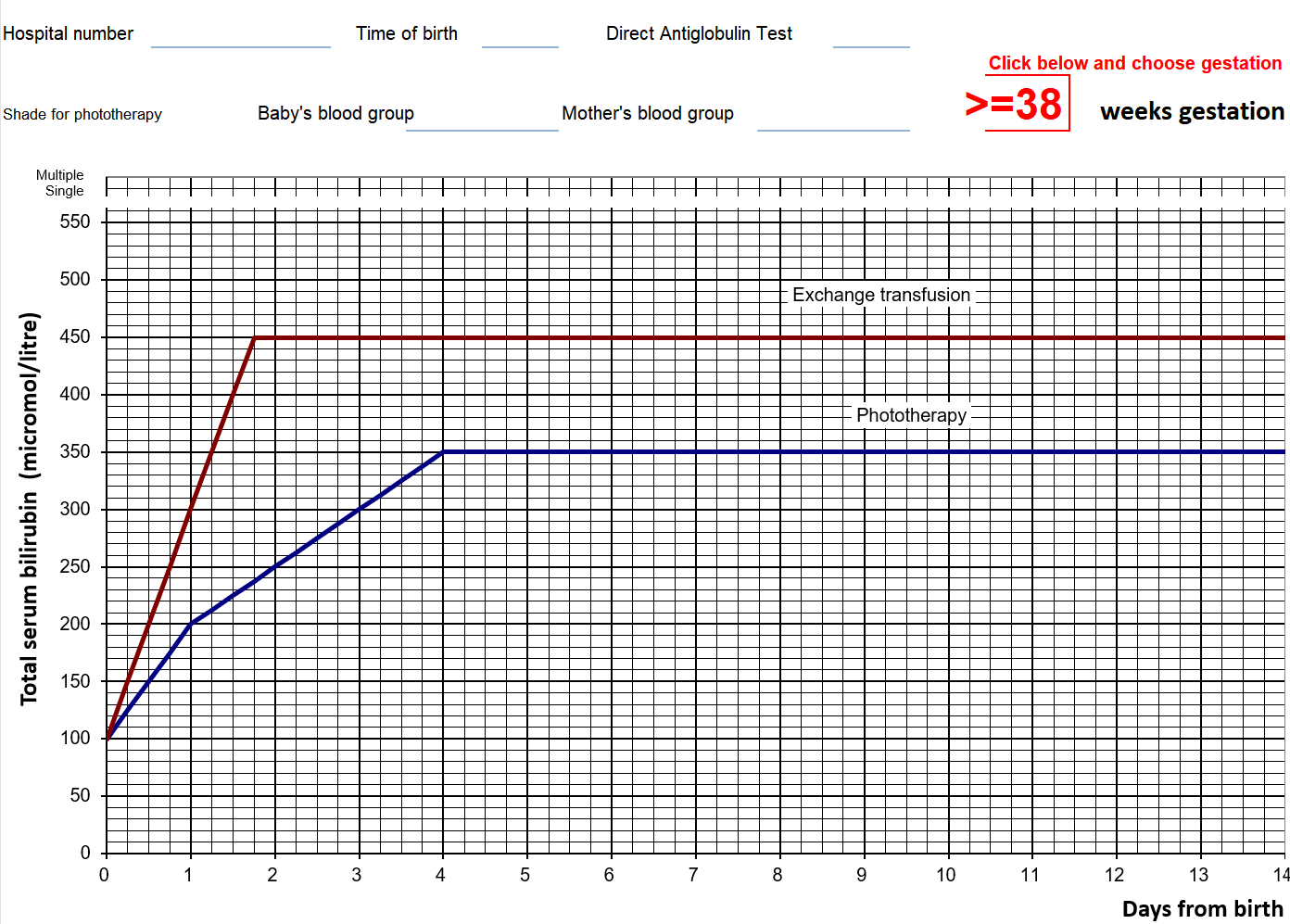
Active management is guided by the treatment threshold graphs (see below for an example)
- Only offer treatment if serum bilirubin level is on / above the treatment line
- If on / above the phototherapy treatment line → start phototherapy
- If on / above the exchange transfusion treatment line → start phototherapy while preparing for exchange transfusion
- If the bilirubin level is below the phototherapy threshold but within 50 mmol/L of the threshold → repeat serum bilirubin measurement within 24 hours (or 18 hours in those with risk factors)
Treatment thresholds (and ongoing monitoring) are based on serum bilirubin level (but not transcutaneous bilirubin measurements).
Treatment Threshold Graph
Treatment graphs for phototherapy/exchange transfusion plot serum bilirubin against post-natal age (different graphs for different gestational ages are available).
The following is an example for ≥38 weeks of gestation.
Phototherapy
| Mechanism | Phototherapy uses artificial blue-spectrum light to convert bilirubin in the skin into water-soluble photoisomers that can be excreted without normal hepatic conjugation.
Do NOT use natural sunlight to deliver phototherapy. |
| Parental education | Educate parents about phototherapy:
|
| Monitoring | Monitor with serum bilirubin level
During phototherapy:
Monitoring after phototherapy:
|
| Intensifying phototherapy | Phototherapy can be intensified by adding another light source or increasing the irradiance of the initial light source
Consider intensifying phototherapy if any of the following:
IV immunoglobulin can be used as an adjunct to intensified phototherapy. Indication:
|
| Stopping phototherapy | Only stop phototherapy when serum bilirubin level is at least 50 mmol/L below the phototherapy treatment line |
Reassure that breastfeeding, nappy‑changing and cuddles can usually continue.
Exchange Transfusion
Exchange transfusion should be performed in a neonatal intensive care bed
- Mechanism: baby’s blood is removed and replaced with donor blood to rapidly reduce the bilirubin level
- Use a double volume exchange transfusion
- Do not stop any ongoing phototherapy while performing exchange transfusion